How Digital Identity Protects Patient Data
Post Summary
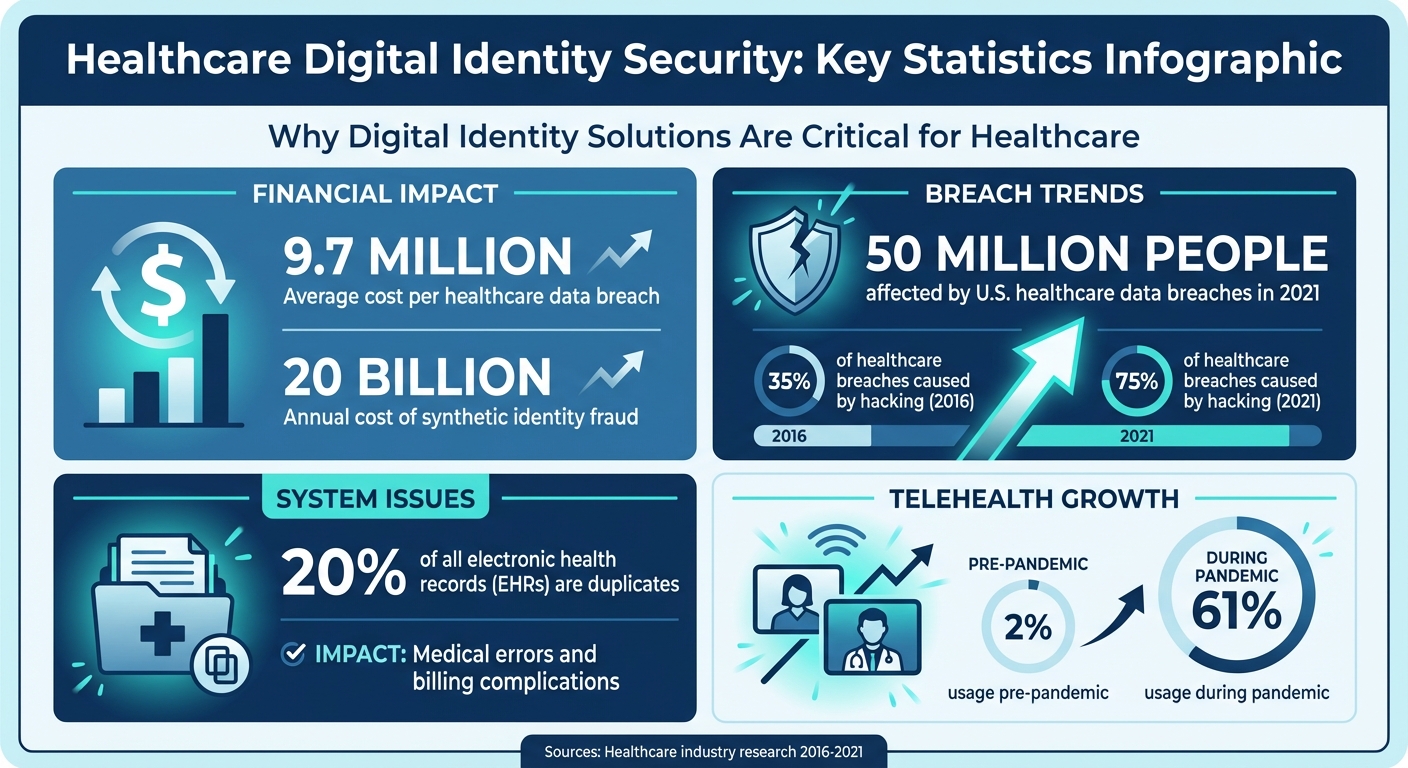
Digital identity in healthcare refers to the secure electronic credentials and verification systems used to confirm the identity of patients and providers, control access to patient data, and enable secure data sharing across clinical systems. Healthcare data breaches average $9.7 million per incident, hacking accounted for nearly 75% of incidents in 2021 — up from 35% in 2016 — and nearly 50 million U.S. individuals were affected by healthcare data breaches in 2021 alone. With remote care usage jumping from 2% pre-pandemic to 61% during the crisis, the patient-facing attack surface has expanded dramatically, making robust digital identity systems a fundamental patient safety and compliance requirement rather than an optional security enhancement.
Biometric authentication — including facial recognition, fingerprint scans, and iris recognition — replaces traditional passwords with physical traits that are extremely difficult to replicate. ISO 30107-certified liveness detection requires real-time user actions such as blinking or smiling to counter deepfakes and static image spoofing. Multi-factor authentication adds an additional layer by combining SMS codes, app-based verification, and biometrics. Adaptive authentication uses risk scoring to flag unusual login behavior and applies additional verification only when behavioral signals suggest elevated risk. Identity proofing matches live selfies to government-issued IDs and cross-references authoritative databases, helping combat synthetic identity fraud — estimated to cost $20 billion annually — and reduce duplicate EHR records, which affect approximately 20% of all electronic health records.
Role-Based Access Control enforces access boundaries by granting permissions based on defined job roles rather than individual user judgment. A billing specialist cannot view clinical notes; a nurse in one department cannot access records from another without explicit clearance. This structure minimizes both insider threats and the blast radius of compromised credentials. Healthcare organizations use Customer Identity and Access Management systems to extend RBAC to the millions of patients accessing records through personal devices — a scale that traditional employee-focused IAM frameworks cannot accommodate. RBAC also supports delegated access, allowing caregivers or designated proxies to manage health information for elderly or disabled patients. NIST Identity Assurance Level 2 and Authenticator Assurance Level 2 standards provide the verification benchmarks that patient portals should meet.
Portable digital credentials allow patients to use a single verified identity across multiple providers, eliminating duplicate accounts and fragmented identity records. FHIR APIs form the technical backbone for interoperable data exchange, enabling verified identities to integrate across different healthcare systems while encryption protects data in transit. OAuth 2.0 and SMART on FHIR provide the secure API authentication layer that prevents unauthorized access during data transfers. The CARIN Alliance promotes a patient-centered model giving individuals control over how and when their health data is shared. Strong access controls, end-to-end encryption, and regular API misconfiguration reviews are essential to preventing PHI exposure during interoperable data exchange.
HIPAA establishes the U.S. standard for safeguarding patient records and healthcare transactions and requires secure authentication, access controls, and audit logging for PHI. GDPR requires organizations handling EU citizen data to report breaches within 72 hours, conduct regular data protection impact assessments, and maintain transparent patient consent processes. The 21st Century Cures Act mandates secure, direct patient access to health data without barriers to electronic health records, creating an interoperability obligation that must be balanced against robust identity and access management. Navigating these overlapping and sometimes conflicting frameworks makes implementing compliant digital identity systems a resource-intensive organizational challenge.
Censinet RiskOps™ provides a unified platform for managing digital identity risks across vendors, clinical applications, and medical devices. Delta-based reassessments reduce vendor reassessment times to less than a day on average by focusing only on changes rather than full reviews from scratch. The Digital Risk Catalog™ provides pre-assessed data on over 50,000 vendors and products. Automated workflows handle audit trails, access revocation, and compliance reporting, with real-time alerts for threats including credential theft and missing Business Associate Agreements. The 1-Click Evidence Sharing feature allows vendors to complete questionnaires once and share them with unlimited customers, and the Censinet Risk Network of over 100 provider and payer facilities enables peer benchmarking of cybersecurity posture including device authentication and supply chain risks.
Healthcare organizations face a growing challenge: protecting sensitive patient data while ensuring seamless access for authorized users. Digital identity solutions are now key to addressing this issue, offering secure ways to verify identities, control access, and share data across platforms. Here's what you need to know:
With healthcare data breaches costing an average of $9.7 million per incident, implementing strong digital identity solutions isn't optional - it's a necessity. The integration of advanced tools, such as Censinet RiskOps™, further streamlines risk management, automates processes, and strengthens security.
This article explores how digital identity works, its core components, and the challenges healthcare organizations face in safeguarding patient data.
Healthcare Data Breach Statistics and Digital Identity Security Impact
Digital ID Flips the Script on Patient Data Ownership
sbb-itb-535baee
Core Elements of Digital Identity in Healthcare
In healthcare, digital identity hinges on three key components: strong authentication, precise access controls, and secure data sharing. These elements work together to safeguard patient information and close gaps in data protection.
Authentication Methods to Block Unauthorized Access
Traditional passwords are increasingly being phased out in healthcare due to their security flaws. Instead, biometric authentication - like facial recognition, fingerprint scans, and iris recognition - has become a core defense. These physical traits are extremely difficult to replicate, making them a reliable barrier against unauthorized access[4][8]. To strengthen this further, technologies like ISO 30107-certified liveness detection ensure real-time user actions (e.g., blinking or smiling) are required, effectively countering deepfakes and static images[4][8].
Multi-factor authentication (MFA) adds another layer of protection by combining methods like SMS codes, app-based verification, and biometrics[6]. For a more seamless experience, adaptive authentication uses risk scoring to flag unusual login behavior, only increasing security measures when necessary. This strikes a balance between user convenience and robust protection.
"Healthcare data's unique sensitivity makes the front-end verification process even more critical, as any failure to accurately confirm identity can lead to unauthorized parties gaining access to personal health records." - ID Dataweb
Identity proofing takes security a step further by matching live selfies to government-issued IDs, such as mobile driver’s licenses, and cross-referencing authoritative databases[4][8]. This approach not only helps combat synthetic identity fraud, which costs an estimated $20 billion annually, but also reduces duplicate records - an issue affecting about 20% of all electronic health records (EHRs). Duplicate records can lead to medical errors and billing complications[4].
Once authentication is secured, the next challenge is defining who can access what data.
Role-Based Access Control (RBAC) Through IAM
Identity and Access Management (IAM) systems ensure that access to patient data is strictly controlled. Unlike traditional IAM frameworks designed for employees, healthcare organizations now rely on Customer Identity and Access Management (CIAM) to handle millions of patients using personal devices[6].
Role-Based Access Control (RBAC) enforces boundaries by granting access based on roles. For example, a billing specialist can’t view clinical notes, and a nurse in one department can’t access records from another without proper clearance. This minimizes insider and third-party threats and limits the damage caused by compromised credentials. RBAC also supports delegated access, allowing caregivers or proxies to manage health information for patients who are elderly or have disabilities[6].
To enhance security and comply with regulations, healthcare organizations are adopting standards like NIST Identity Assurance Level 2 (IAL2) and Authenticator Assurance Level 2 (AAL2) for patient portals[7][9]. These standards provide clear guidelines for verification processes while maintaining ease of use.
With access tightly controlled, the next priority is ensuring secure data sharing across systems.
Secure Data Sharing Between Providers
As patients move between specialists, hospitals, and telehealth platforms, their data must travel securely alongside them. Portable digital credentials allow patients to use a single, verified identity across multiple providers, eliminating the need for multiple accounts[7][9]. The CARIN Alliance promotes this patient-centered model, giving individuals control over how and when their data is shared[7].
FHIR (Fast Healthcare Interoperability Resources) APIs form the technical backbone for this interoperability, enabling verified identities to integrate seamlessly across different healthcare systems[9]. Encryption ensures data remains secure during these transfers.
The importance of secure sharing is underscored by the scale of breaches: in 2021, nearly 50 million people in the U.S. were affected by healthcare data breaches, with hacking responsible for nearly 75% of incidents - up from 35% in 2016[7]. The rapid rise of remote care, which jumped from 2% usage pre-pandemic to 61% during the crisis, has further expanded the attack surface[8].
Challenges in Protecting Patient Data
Healthcare data breaches come with hefty consequences - financial losses, damaged reputations, and regulatory penalties. On average, these breaches cost a staggering $9.7 million, making them a serious concern for healthcare organizations.
Data Breach Risks and Vulnerabilities
Healthcare systems face persistent threats like credential theft and insider attacks. The widespread adoption of cloud platforms, electronic health records (EHRs), and telemedicine has expanded the potential points of attack, including vulnerable medical devices. This broader digital footprint leaves labs, hospitals, insurance providers, and even government databases more exposed to cyber risks[2]. To counter these threats, advanced digital identity protections are critical.
Balancing Interoperability with Security
Efficient data sharing is vital in healthcare, but ensuring this exchange happens securely is a tough balancing act. Frameworks like GS1 identifiers and HL7 FHIR promote secure data sharing, but integrating these standards with strong access controls isn’t straightforward[2]. On top of that, outdated verification processes can hinder patient access while also raising privacy concerns.
Compliance with Changing Regulations
Digital identity systems must incorporate secure authentication and access controls to align with various regulatory demands. However, navigating these overlapping frameworks is no small feat. For instance:
Managing sensitive healthcare data under these complex and sometimes conflicting regulations makes implementing secure digital identity systems a resource-heavy challenge[3].
How Censinet RiskOps™ Strengthens Digital Identity Security
Managing digital identity risks in healthcare is no small task. Threats evolve quickly, and keeping up requires tools that can adapt just as fast. That's where Censinet RiskOps™ steps in, offering a unified platform that connects IT, biomedical, supply chain, and research departments to streamline risk management.
Faster Risk Assessments
Traditional risk assessments can stretch on for weeks, leaving organizations vulnerable in the meantime. Censinet RiskOps™ speeds up the process using delta-based reassessments. Instead of reviewing all vendor data from scratch, it focuses only on changes in responses, cutting reassessment times to less than a day on average[10]. Plus, its Digital Risk Catalog™ provides instant access to over 50,000 pre-assessed vendors and products, making it easier to evaluate digital identity solutions efficiently[10].
Terry Grogan, CISO at Tower Health, shared how this efficiency transformed their operations:
"Censinet RiskOps allowed 3 FTEs to go back to their real jobs! Now we do a lot more risk assessments with only 2 FTEs required."
Automated Cybersecurity Workflows
Manually tracking security gaps is not only time-consuming but also risky - delays can give attackers a window of opportunity. Censinet RiskOps™ eliminates these delays by automating key workflows, including audit trails, access revocation, and compliance reporting. The platform sends real-time alerts for threats like credential theft and flags issues such as missing Business Associate Agreements (BAAs) or vulnerabilities like Log4j across the vendor portfolio. Automated Corrective Action Plans (CAPs) ensure teams can address these gaps quickly and effectively[10].
This level of automation fosters a more seamless and collaborative approach to managing digital identity risks, saving time while enhancing security.
Collaborative Risk Management for HDOs
Digital identity security isn't just an IT issue - it’s a team effort involving clinical staff, vendors, and leadership. Censinet RiskOps™ acts as a hub for collaboration, enabling healthcare delivery organizations (HDOs) and third-party vendors to share cybersecurity data efficiently. The platform’s 1-Click Evidence Sharing feature allows vendors to complete standardized questionnaires once and share them instantly with unlimited customers, ensuring data stays current[10].
With over 100 provider and payer facilities participating in the Censinet Risk Network, organizations can benchmark their cybersecurity efforts against peers. This collaborative environment helps identify shared vulnerabilities in areas like device authentication and supply chain risks[10].
Best Practices for Implementing Digital Identity Solutions
Creating an effective digital identity strategy requires careful planning. It should address risks, accommodate future growth, and establish secure, unified practices.
Conduct Regular Risk Assessments
Hoping for the best isn't a plan. Regular risk assessments - ideally every quarter or after major system updates - are essential for spotting issues before they escalate. Keep an eye on unauthorized access, use AI to detect anomalies, and review healthcare cybersecurity benchmarking and compliance audits thoroughly.
Adopt Identity and Access Management (IAM) frameworks with built-in audit trails for continuous oversight. Incorporating standards like HL7 FHIR ensures that security measures align with data-sharing needs and regulatory requirements[2][3]. The aim is clear: identify threats early, fix vulnerabilities quickly, and stay HIPAA-compliant.
This proactive approach sets the stage for implementing technologies that can grow alongside your organization.
Adopt Scalable, Compliant Technologies
Your digital identity solutions need to grow with you. Scalable technologies like multi-factor authentication (MFA), biometrics, and Zero Trust Architecture provide ongoing verification and adaptability. Look for tools with features like end-to-end encryption, liveness detection to block spoofing, and adaptive role-based access control that adjusts as your organization evolves.
Real-world examples show that dynamic identity verification can reduce fraud, cut down errors, and simplify patient onboarding and access to electronic health records. Choosing technologies that balance scalability with compliance ensures your security measures can keep up with changing regulations and organizational needs.
But even the best technology won't work without a knowledgeable team.
Train Staff on Secure Practices
Technology isn't enough if your team doesn't know how to use it securely. Annual training sessions, supplemented by quarterly refreshers, help staff identify threats like phishing, properly use MFA and biometrics, understand role-based access control, and respond to access log alerts[2][3]. Since human error often leads to breaches, ongoing education is essential.
Training should be practical, not just theoretical. Staff who can spot credential theft, confidently use biometric systems, and report anomalies become a critical part of your defense. The key is to integrate these practices into daily routines rather than limiting them to occasional compliance checks.
Conclusion
Digital identity serves as the backbone for safeguarding patient data in today's interconnected healthcare environment. With the steep financial and reputational costs of data breaches, healthcare organizations can no longer rely on outdated authentication methods. By adopting digital identity frameworks that integrate multi-factor authentication, biometrics, and Zero Trust Architecture, organizations can tackle key vulnerabilities like unauthorized access, credential theft, and compliance risks.
However, the challenge isn't just about deploying advanced authentication tools - it’s also about managing the complexity that comes with integrating these solutions across various vendors, clinical applications, and medical devices. This is where Censinet RiskOps™ steps in. Designed specifically for healthcare delivery organizations, it simplifies risk assessments, automates cybersecurity workflows, and supports collaborative risk management. As the first cloud-based risk exchange tailored for healthcare, it offers the visibility and control needed to safeguard PHI while adhering to HIPAA requirements[11].
Emerging technologies are also paving the way for even stronger data protection measures. Innovations like AI-driven verification, blockchain-based patient-controlled identities, and dynamic risk-based authentication are transforming how healthcare organizations secure access to sensitive information[2][5]. By combining these advancements with established digital identity frameworks and solutions like Censinet RiskOps™, healthcare organizations can stay ahead of evolving threats while meeting regulatory demands, including those outlined in the 21st Century Cures Act.
FAQs
What’s the difference between authentication and identity proofing?
In the world of digital identity management, identity proofing plays a crucial role during account setup. This process verifies a person’s identity by using documents such as government-issued IDs or biometrics, helping to prevent fraudulent activities. Importantly, this step happens just once during the onboarding phase.
On the other hand, authentication is an ongoing process. It ensures a user’s identity is confirmed every time they access a system. This is typically done through methods like passwords, multi-factor authentication (MFA), or biometrics.
Together, these processes work to safeguard sensitive patient data and ensure compliance with healthcare regulations, such as HIPAA.
How does RBAC limit what staff can see in EHRs?
RBAC, or Role-Based Access Control, limits staff access to Electronic Health Records (EHRs) by assigning permissions based on their specific job roles. This approach ensures that only the right personnel can view or interact with certain patient data. By restricting access in this way, RBAC helps reduce the chances of data breaches, making it easier to maintain HIPAA compliance. It’s a practical way to enhance data security while meeting healthcare's strict regulatory standards.
How can providers share data via FHIR without risking PHI?
Providers can share data securely using FHIR by leveraging secure APIs equipped with strong authentication methods like OAuth 2.0 and SMART on FHIR. To protect patient health information (PHI) and meet healthcare regulations, it's crucial to follow key practices such as:
These steps are essential for maintaining the integrity and security of sensitive healthcare data.
Related Blog Posts
- HIPAA Compliance and Biometric Data in Clinical Apps
- How IAM Integration Prevents Healthcare Data Breaches
- Telehealth Security: Identity Proofing vs. Authentication
- HIPAA Standards for Digital Identity
{"@context":"https://schema.org","@type":"FAQPage","mainEntity":[{"@type":"Question","name":"What’s the difference between authentication and identity proofing?","acceptedAnswer":{"@type":"Answer","text":"<p>In the world of digital identity management, <strong>identity proofing</strong> plays a crucial role during account setup. This process verifies a person’s identity by using documents such as government-issued IDs or biometrics, helping to prevent fraudulent activities. Importantly, this step happens just once during the onboarding phase.</p> <p>On the other hand, <strong>authentication</strong> is an ongoing process. It ensures a user’s identity is confirmed every time they access a system. This is typically done through methods like passwords, multi-factor authentication (MFA), or biometrics.</p> <p>Together, these processes work to safeguard sensitive patient data and ensure compliance with healthcare regulations, such as HIPAA.</p>"}},{"@type":"Question","name":"How does RBAC limit what staff can see in EHRs?","acceptedAnswer":{"@type":"Answer","text":"<p>RBAC, or Role-Based Access Control, limits staff access to Electronic Health Records (EHRs) by assigning permissions based on their specific job roles. This approach ensures that only the right personnel can view or interact with certain patient data. By restricting access in this way, RBAC helps reduce the chances of data breaches, making it easier to maintain HIPAA compliance. It’s a practical way to enhance data security while meeting healthcare's strict regulatory standards.</p>"}},{"@type":"Question","name":"How can providers share data via FHIR without risking PHI?","acceptedAnswer":{"@type":"Answer","text":"<p>Providers can share data securely using FHIR by leveraging secure APIs equipped with strong authentication methods like <strong><a href=\"https://oauth.net/2/\" target=\"_blank\" rel=\"nofollow noopener noreferrer\">OAuth 2.0</a></strong> and <strong><a href=\"https://smarthealthit.org/\" target=\"_blank\" rel=\"nofollow noopener noreferrer\">SMART on FHIR</a></strong>. To protect patient health information (PHI) and meet healthcare regulations, it's crucial to follow key practices such as:</p> <ul> <li><strong>Strong access controls</strong>: Limit access to authorized users only.</li> <li><strong>Data encryption</strong>: Encrypt data both in transit and at rest.</li> <li><strong>Addressing API misconfigurations</strong>: Regularly review and fix potential vulnerabilities to prevent breaches.</li> </ul> <p>These steps are essential for maintaining the integrity and security of sensitive healthcare data.</p>"}}]}
Key Points:
Why has traditional password-based authentication become inadequate for healthcare and what replaces it?
- Passwords cannot scale to the healthcare identity challenge — Healthcare organizations manage identity for clinical staff, administrative personnel, patients, and external vendors simultaneously. Passwords are reused, shared, phished, and stolen at scale — and the healthcare sector's high-value patient data makes it a primary target for credential theft attacks that passwords cannot reliably resist.
- Biometrics provide inherently non-transferable authentication — Facial recognition, fingerprint scans, and iris recognition authenticate based on physical traits that cannot be shared, guessed, or stolen through phishing. These biometric modalities are difficult to replicate and provide a reliable first-factor authentication layer for both clinical staff and patient-facing systems.
- ISO 30107-certified liveness detection counters deepfake attacks — As AI-generated deepfakes and high-quality static images become capable of defeating basic facial recognition systems, ISO 30107-certified liveness detection requires real-time user actions — blinking, smiling, or head movement — to confirm that the authentication subject is a live person rather than a presented artifact.
- MFA layers verification methods for defense-in-depth authentication — Multi-factor authentication combines two or more verification methods — something the user knows, has, or is — so that compromising any single factor does not enable access. SMS codes, app-based TOTP verification, hardware tokens, and biometrics can be combined to match the sensitivity of the data being accessed.
- Adaptive authentication balances security with clinical workflow efficiency — High-friction authentication that applies maximum verification at every login creates workflow delays that clinical staff under time pressure will circumvent. Adaptive authentication uses real-time risk scoring based on behavioral signals — unusual access times, unfamiliar devices, anomalous data requests — to apply enhanced verification only when risk indicators warrant it.
- Identity proofing addresses synthetic fraud and duplicate EHR records — Live selfie-to-government-ID matching cross-referenced against authoritative databases addresses synthetic identity fraud estimated at $20 billion annually and reduces the duplicate EHR records that affect approximately 20% of electronic health records — duplicate records that create medication error risks and billing complications that go beyond cybersecurity into direct patient safety consequences.
How does Role-Based Access Control through IAM and CIAM architectures protect patient data at enterprise and patient scale?
- RBAC enforces the minimum necessary standard operationally — HIPAA's minimum necessary standard requires that access to PHI be limited to what each workforce member needs to perform their specific job function. RBAC implements this standard as a technical control rather than a behavioral expectation, ensuring that a billing specialist cannot access clinical notes and a nurse in one ward cannot access records from another department without explicit authorization.
- CIAM extends access management to millions of patient-device combinations — Traditional enterprise IAM is designed for a finite employee population using organizational devices. Healthcare patient populations using personal smartphones, tablets, and home computers to access portals, telehealth platforms, and health apps require Customer Identity and Access Management architectures that scale to millions of concurrent identities across heterogeneous device environments.
- Delegated access addresses caregiving and proxy scenarios — RBAC in healthcare must accommodate delegated access — the structured ability for caregivers, legal guardians, and designated proxies to manage health information for patients who are elderly, have disabilities, or are minors. This delegation must be authorized, documented, and revocable, adding governance complexity beyond the standard employee role model.
- NIST IAL2 and AAL2 provide compliance benchmarks for patient portals — NIST Identity Assurance Level 2 and Authenticator Assurance Level 2 establish standardized requirements for identity verification and authentication strength that patient portals should meet to satisfy both HIPAA technical safeguard requirements and the secure access obligations of the 21st Century Cures Act.
- Insider threat reduction through access boundary enforcement — Insider threats — whether malicious or inadvertent — represent a significant share of healthcare data breach incidents. RBAC limits the data accessible to any individual credential to their role scope, ensuring that a compromised or misused credential cannot reach data outside that role's authorized domain and limiting the blast radius of insider incidents.
- IAM audit trails as a HIPAA compliance and breach investigation tool — IAM systems generate access logs that record who accessed what data, when, from which device, and through which authentication method. These audit trails satisfy HIPAA's audit control technical safeguard requirement and serve as the primary forensic tool for breach investigation, enabling organizations to identify what data was accessed and by whom during a security incident.
What technical infrastructure supports secure interoperable data sharing across healthcare providers while protecting PHI?
- FHIR APIs as the interoperability backbone — Fast Healthcare Interoperability Resources APIs provide the standardized technical interface that enables verified patient identities to move securely across different healthcare systems — from primary care to specialist to hospital to telehealth — without requiring each system to maintain separate identity records or authentication credentials for the same patient.
- OAuth 2.0 and SMART on FHIR for secure API access — OAuth 2.0 provides the authorization framework that governs which applications can access which FHIR resources on behalf of which authenticated users. SMART on FHIR extends this framework specifically for healthcare application ecosystems, enabling patient-authorized third-party applications to access EHR data through standardized, permission-scoped API calls without exposing underlying PHI to unauthorized systems.
- Portable digital credentials eliminate identity fragmentation — When patients move between specialists, hospitals, pharmacies, and telehealth platforms, maintaining separate accounts for each creates both security vulnerabilities — from password reuse and account abandonment — and care quality risks from fragmented records. Portable digital credentials allow a single verified identity to travel with the patient across all care settings.
- Encryption in transit as a non-negotiable data sharing control — All PHI transmitted through FHIR APIs or any other interoperability mechanism must be encrypted in transit to prevent interception. End-to-end encryption ensures that data remains protected between the originating system and the authorized recipient, regardless of the network infrastructure through which it travels.
- API misconfiguration as a primary PHI exposure vector — Properly implemented FHIR APIs with strong authentication do not inherently expose PHI. API misconfigurations — overly permissive scopes, missing authentication requirements, inadequate rate limiting — are the primary vector through which secure-by-design APIs become PHI exposure risks. Regular API security reviews and automated misconfiguration detection are essential maintenance requirements.
- CARIN Alliance patient-centered data sharing model — The CARIN Alliance promotes a patient-controlled data sharing model in which individuals have explicit authority over how and when their health information is shared across providers and applications, aligning digital identity infrastructure with the patient data rights that the 21st Century Cures Act establishes and the patient trust that HIPAA was designed to protect.
What are the primary challenges healthcare organizations face when implementing digital identity systems and how should they be addressed?
- Expanding attack surface from cloud, EHR, and telehealth adoption — The broad adoption of cloud platforms, electronic health records, and telemedicine has multiplied the entry points available to attackers, including vulnerable medical devices, patient portals, remote access infrastructure, and third-party application integrations. Each new connected system introduces identity and access management requirements that legacy authentication approaches were not designed to address.
- Balancing interoperability with access control — Frameworks like GS1 identifiers and HL7 FHIR promote the secure data sharing that care coordination requires, but integrating these standards with granular access controls — ensuring that data flows to authorized systems and users without creating new exposure pathways — requires careful architecture and ongoing governance that is technically demanding and organizationally complex.
- Navigating overlapping and sometimes conflicting regulatory frameworks — Healthcare organizations operating under HIPAA, GDPR, the 21st Century Cures Act, and state-level privacy laws face compliance obligations that vary in specific requirements and sometimes create tensions — for example, GDPR's right to erasure versus HIPAA's records retention requirements. Digital identity systems must be designed to satisfy multiple regulatory frameworks simultaneously without creating compliance gaps in any.
- Outdated verification processes that create friction without providing security — Verification processes based on knowledge-based authentication — secret questions, date of birth, last four digits of Social Security number — are widely available in data breach repositories and provide minimal security while creating patient friction. Replacing these with document-verified identity proofing and biometric authentication requires significant workflow redesign but produces security improvements that knowledge-based methods cannot match.
- Legacy system integration complexity — Healthcare organizations operate technology environments spanning multiple decades of system generations. Integrating modern digital identity and access management infrastructure with legacy clinical systems that were not designed with API-based authentication in mind requires middleware solutions, custom integrations, and extended implementation timelines that strain IT capacity.
- Human error as the persistent vulnerability underlying all technical controls — The most sophisticated digital identity infrastructure can be undermined by staff who share credentials, fail to report suspicious access requests, or bypass security measures under time pressure. Annual training supplemented by quarterly refreshers on phishing recognition, proper MFA use, RBAC boundaries, and access log anomaly reporting converts the human layer from a vulnerability into a detection asset.
What emerging technologies are reshaping healthcare digital identity and what is their patient data protection potential?
- AI-driven identity verification accelerates and strengthens proofing — AI-driven verification systems analyze document authenticity, biometric consistency, and behavioral patterns at speeds and accuracy levels that manual verification cannot match, enabling real-time identity proofing for patient onboarding and remote care access without the delays that document review processes traditionally impose.
- Blockchain-based patient-controlled identity models — Blockchain technology enables decentralized identity architectures in which patients hold and control their own verified identity credentials rather than depending on any single healthcare organization or identity provider. This patient-controlled model eliminates centralized identity repositories as single points of compromise and aligns with the patient data ownership principles that emerging regulations increasingly support.
- Dynamic risk-based authentication replaces static verification tiers — Rather than applying a fixed authentication level to all accesses within a permission tier, dynamic risk-based authentication continuously reassesses risk based on real-time behavioral signals and adjusts verification requirements within an active session — providing stronger protection during anomalous behavior without imposing unnecessary friction during normal workflow.
- Zero Trust Architecture as the identity-centric security framework — Zero Trust Architecture treats every access request as untrusted regardless of network location, requiring continuous identity verification, device validation, and least-privilege access enforcement for every resource request. In healthcare environments where trusted internal networks have repeatedly proven insufficient to contain breaches, ZTA provides the architectural shift that makes identity the new security perimeter.
- Synthetic identity fraud and deepfake threat evolution — The $20 billion annual cost of synthetic identity fraud and the accelerating sophistication of AI-generated deepfake attacks establish that digital identity threats are not static. ISO 30107-certified liveness detection, continuous behavioral monitoring, and AI-powered anomaly detection must evolve alongside these threats to maintain their protective effectiveness.
- Interoperability between digital identity systems across health ecosystems — As patient care increasingly spans multiple organizations, states, and countries, digital identity systems must achieve interoperability not only for clinical data but for the identity credentials themselves. Standards-based portable credential frameworks that enable a verified identity established at one organization to be recognized and trusted at another represent the next frontier of digital identity infrastructure for healthcare.
How does Censinet RiskOps™ specifically address the vendor risk, automation, and collaborative oversight requirements that digital identity management in healthcare demands?
- Delta-based reassessment reducing vendor review time to under a day — Traditional vendor risk assessments reviewing all data from scratch consume weeks of analyst time. Censinet RiskOps™'s delta-based reassessment approach focuses exclusively on changes in vendor responses since the last assessment, reducing reassessment time to less than a day on average and enabling continuous vendor oversight rather than periodic snapshots.
- Digital Risk Catalog™ with 50,000+ pre-assessed vendors — The Digital Risk Catalog™ provides instant access to pre-assessed security profiles for over 50,000 vendors and products, enabling healthcare organizations to evaluate digital identity solution vendors, authentication technology providers, and IAM platform vendors against existing risk data rather than initiating assessments from scratch for every new vendor evaluation.
- Real-time alerts for credential theft and missing BAAs — Automated real-time alerts for threats including credential theft, missing Business Associate Agreements, and known vulnerabilities such as Log4j across the vendor portfolio provide the continuous monitoring that manual oversight cannot sustain — closing the gap between annual assessments and the continuous threat activity that healthcare organizations face.
- Automated Corrective Action Plans for gap remediation — Automated CAPs ensure that identified security gaps — including access control deficiencies, missing authentication requirements, and vendor compliance failures — are assigned to responsible parties with documented timelines, converting risk identification into structured remediation rather than untracked findings.
- 1-Click Evidence Sharing enabling vendor compliance at scale — The 1-Click Evidence Sharing feature allows vendors to complete standardized security questionnaires once and share them instantly with unlimited healthcare organization customers, maintaining currency of shared data while eliminating the redundant questionnaire completion burden that traditional vendor assessment processes impose.
- Censinet Risk Network benchmarking across 100+ provider and payer facilities — The Censinet Risk Network enables healthcare organizations to benchmark their cybersecurity posture — including digital identity controls, device authentication practices, and supply chain risks — against peer institutions, providing the comparative context that internal assessment alone cannot supply and supporting evidence-based security investment decisions.

